|
Rotation Policies & Procedures
MICU/CCU
Last Updated: 12/13/18
New and Updated sections are in red
I. Guidelines and Policies
II. Rotation Logistics
I. Guidelines and Policies Medical Intensive Care Unit A. Admission Workflow
- ED Admissions
- ED resident/attending will evaluate patient for possible admission to ICU based on specific needs, e.g. mechanical ventilation, vasopressor or other titrable drips, clinical status, risk of further decompensation
- In situations where need for ICU level of care is unclear, ED will request evaluation from MICU team regarding need for admission
- MICU senior resident will evaluate patient for possible admission to ED in discussion with MICU fellow and/or attending
- MICU resident will document evaluation and recommendations in EPIC for all patients deemed not to require ICU care
- ED resident/attending will place bed request and page MICU team for admission
- MICU intern/resident will evaluate patient in ED and place appropriate admission orders.
- Outside Hospital Transfers
- MICU attending intensivist will review and accept all transfers to UCI MICU. Attending will notify team of incoming transfers as appropriate
- MICU team may request records, as appropriate, from Transfer Center (x2222) for all incoming transfers
- MICU team will be notified by nursing once patient arrives in ICU. MICU team will place admission orders and make appropriate documentation
- In event patient does not arrive prior to signout, MICU team will place initial admission orders and start initial H&P note. Admission will be completed by MICU night float resident once patient arrives.
- Rapid Response/Code Blue
- MICU senior resident will carry RRT/Code Blue pager at all times during day hours (6:00AM-6:00PM)
- MICU senior resident (along with Team H resident) will respond to all RRT and Code Blue called in hospital
- Following RRT or Code Blue, either MICU senior resident or Team H resident will document events in EPIC
B. Admission Criteria
- Head Injury/Bleed
- MICU service
- Isolated non-operative traumatic brain injury without intracranial hemorrhage, with multiple medical comorbidities, age >75yrs or syncope (May also be admitted to Hospitalist service based on clinical status)
- Isolated non-operative traumatic brain injury with minor intracranial hemorrhage with mulitple medical comorbidities, age>75yrs, or syncope, with definitive and rapid recommendations from Neurosurgery service.
- Trauma service
- Multisystem trauma patient with operative or non-operative head injury. Multisystem does not include patients with skull, C-spine, facial fractures or minor torso trauma.
- Isolated non-operative mild traumatic brain injury (GCS 13-15) patient without significant co-morbidities.
- Neurosurgery service
- Isolated operative traumatic intracranial hemorrhage patients. “Isolated” includes patients with skull, C-spine, facial fractures, and minor torso trauma.
- Isolated non-operative significant traumatic intracranial hemorrhage requiring repeat CT scans or IR interventions. Includes patients who undergo or are at significant risk to undergo craniotomy or ICP placement, or who have a GCS < 12.
- Isolated non-operative traumatic brain injury with significant ICH with multiple co-morbidities/age>75 or syncope.
- Spontaneous operative intracranial hemorrhage without significant multisystem injury.
- Spontaneous non-operative intracranial hemorrhage.
- Neuro-Critical Care service
- Seizure related Isolated traumatic brain injury (either pre-trauma or as the significant issue post trauma).
C. Caps
- Intern: Each intern is capped at 6 patients
- Seniors: Each senior is capped at 10 patients
- Additional patients will be managed by ICU fellow
D. Ward Transfers
- ICU follows a "closed ICU" policy. All patients physically in ICU are responsibility of MICU team
- Once patient is ready to be transferred out of ICU, MICU team will place transfer orders to notify SPPO of need for medicine bed
- MICU resident is responsible for determining and notifying SPPO if patient is a bounceback to Hospitalist team or Family Medicine service.
- MICU team will continue to manage patient as primary service (unless Open ICU policy in effect, see below) until bed is assigned
- Once bed is assigned, MICU team will sign out to appropriate Hospitalist team per SPPO.
- If bed is assigned overnight, MICU team will sign out to appropriate Hospitalist team the following morning
- Once signout is complete, Hospitalist team will assume primary responsibility for patient, even if physically still in MICU awaiting transport to floor
- Primary responsibility of patient overnight will depend on their location at time of ward team signout (5:00PM)
- If patient is still in MICU at 5:00PM, they will be managed by MICU night float team
- If patient is on floor at 5:00PM, they will be managed by Wards night float crosscover resident
- Regardless of who has primary responsibility, patient should be signed out to both MICU and Ward night float teams to ensure appropriate continuity of care
E. Fellow/Faculty Escalation Policy NEW
- MICU fellow and/or attending should be contacted for any of the following events on MICU patients:
- Any new ICU Admission
- Any new ICU Consult
- Any significant neurological changes, e.g. seizure, new neurologic deficit, CVA, worsening encephalopathy/unresponsiveness/obtunded state.
- Any new or worsening respiratory failure requiring initiation of 100% FIO2
- Intubation or institution of non-invasive positive pressure ventilation (NIPPV)
- Any worsening hemodynamic instability requiring vasopressor initiation or escalation of multiple vasopressors.
- Any new unstable arrhythmia
- Cardiac arrest
- Death
- Any Discharge Against Medical Advice (AMA)
- If nurse or other physician requests attending notification
F. Open ICU Policy
- In event MICU census is >=18, MICU resident may contact chief resident on-call to temporarily convert to open ICU
- When open ICU policy is in effect, Hospitalist teams will assume primary responsibility of patients awaiting transfer even while still physically in ICU and awaiting bed assignment
- Decision to institute open ICU policy at discretion of on-call chief resident and program director
G. ICU Procedure Policy
- Residents must have verification of procedure competency to perform any and all procedures independently in the ICU
- Procedures requiring verification include (but are not limited to): internal jugular, subclavian and femoral central line; radial and femoral arterial line; lumbar puncture; abdominal paracentesis; and thoracentesis
- In all other cases, resident must be supervised by senior resident, fellow or attending
- Procedure competency determined by successful completion of five (5) attempts independently, and under supervision of competent instructor
- Procedure competency verification will be updated biannually, at fall and spring semi-annual reviews. Residents who achieve competency in procedures in between these dates should contact program coordinator to update status
- Procedure competency logs are maintained on Intranet under Resident Competencies. Resident may only perform those procedures independently listed on this site.
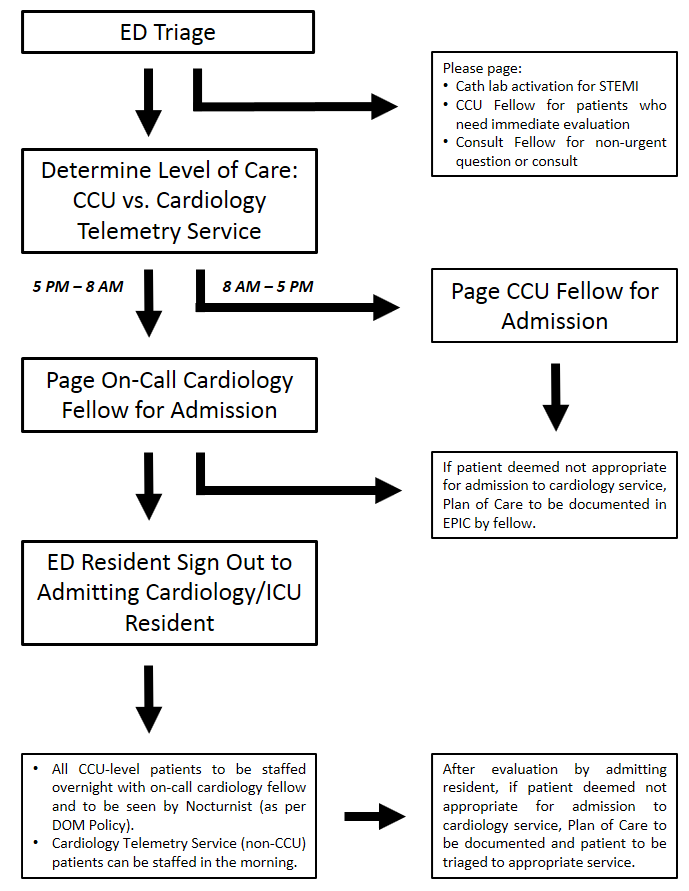
Cardiac Care Unit (CCU) A. Admission Workflow
- ED resident will evaluate patient for possible admission to Cardiology service (including both telemetry and CCU level of care) based on Cardiology admission criteria (see below).
- ED resident will contact appropriate Cardiology fellow for acceptance to Cardiology service. Medicine residents cannot accept patients to Cardiology service, and should not be contacted prior to approval from fellow
- 8AM-5PM: CCU Fellow
- 5PM-8AM: On-Call Cardiology Fellow
- Once Cardiology fellow has accepted patient to Cardiology service, ED resident will contact admitting Medicine resident for signout.
- Any patients deemed not appropriate for admission to Cardiology service by fellow will require Plan of Care documentation in EPIC, with further recommendations, if appropriate.
- For daytime admissions:
- Patients will be staffed with daytime Cardiology service attending per usual schedule
- For overnight admissions:
- Admitting Medicine resident will contact on-call Cardiology fellow to staff all CCU level admissions
- Non-CCU (telemetry) level patients may be staffed by primary team in the morning. However, residents are encouraged to contact on-call Cardiology fellow with any questions that arise.
- Nocturnist will also see all CCU level patients per Department of Medicine policies
B. Admission Criteria
- Cardiology Service (CCU or Telemetry)
- Newly identified acute heart failure decompensation without other acute noncardiac medical problems
- NYHA class III-IV heart failure considered having high in-hospital mortality (BUN>43, SBP<115, and serum Cr>2.75 (excluding patients with CRF or on hemodialysis))
- Suspected or diagnosed acute coronary syndrome (unstable angina, acute myocardial infarction, aborted sudden cardiac death)
- Newly identified and/or potential life-threatening symptomatic arrhythmia (sustained ventricular tachycardia, high-grade atrioventricular block, symptomatic atrial fibrillation, persistent symptomatic brady- or tachyarrhythmia
- Acute decompensated heart failure requiring or at risk of requiring invasive ventilatory support
- Cardiogenic shock or otherwise requiring chemical or mechanical circulatory support (dopamine, dobutamine, milrinone or adrenergic agonist drip, IABP counterpulsation, LVAD)
- Patient regularly followed by member of Cardiology department and without other acute noncardiac medical problem.
- "Regularly followed" defined as two clinic visits within last 12 months
- "Without other acute noncardiac medical problem" defined by best clinical judgment and decision of ED attending
- Medical ICU Service
- Multisystem organ failure
- Requiring or at risk of requiring invasive ventilatory support, excluding acute decompensated heart failure
- Hospital Medicine
- Acute decompensated heart failure not meeting any of above admission criteria, with Cardiology Nurse Practitioner consult
- Following patients, with consideration for urgent Cardiology consultation:
- Persistent or worsening symptoms despite aggressive and sustained intervention.
- Diastolic dysfunction of unclear etiology.
- Inodilator or vasodilator infusion with worsening of heart failure.
- Suspected acute coronary syndrome (i.e. unstable angina, acute myocardial infarction, aborted sudden cardiac death, unexplained abnormal cardiac enzymes).
- Suspected significant coronary artery disease who are candidates for diagnostic angiography/percutancous or surgical coronary intervention.
- Abnormal provocative stress-test who are candidates for diagnostic angiography/percutaneous or surgical coronary intervention.
- Undergoing evaluation for or post cardiac transplant
- Newly identified serious arrhythmias (e.g. ventricular tachycardia, symptomatic brady or tachyarrhythmias, high grade a-v block).
- Destabilized chronic/known arrhythmias.
- Implanted mechanical devices (e.g. LVADs).
- Implanted electrical devices that require interrogation or are suspected of malfunction (e.g. pacemaker, AICD)
- Candidates for cardiac resynchronization (i.e persistent symptoms + EF <35% + QRS interval > .12 sec).
- Currently regularly followed by a member of the Cardiology department (as defined above)
- For evaluation for transfer to Cardiology service
- Readmission/Bouncebacks
- Heart failure patients readmitted within 30 days should be readmitted under the previous team unless condition requires different admission services as best decided by clinical judgment of ED attending
C. ICU Procedure Policy
- All procedures performed on CCU rotation follow same policy as in MICU
- See ICU Procedure Policy under Medical Intensive Care Unit (MICU) above
MICU/CCU Night Float A. Admission Workflow
- Cross-Coverage
- Night float intern and resident will receive signout from day CCU and ICU teams at 6:00PM each evening
- Night float intern will have primary responsibility for cross-coverage of existing patients, with assistance, as needed, from senior resident
- MICU Admissions
- ED resident/attending will evaluate patient for possible admission to ICU.
- As during day, MICU night float resident may also be asked to evaluate patients for possible ICU admission.
- Night float resident will review all evaluations with MICU nocturnist. For any patients deemed to not require ICU admission, resident will document evaluation, recommendations in EPIC
- ED resident/attending will page MICU resident once decision has been made to admit patient
- MICU resident will evaluate patient, place admission orders and write documentation for each admission
- MICU resident will staff all admissions with ICU nocturnist. Nocturnist may see patients together with resident, or independently, at their discretion.
- MICU resident will also staff all admissions with on-call ICU fellow at time of admission.NEW
- CCU Admissions
- ED resident/attending will evaluate patient for possible admission to Cardiology service(including CCU and telemetry)
- ED will contact on-call Cardiology fellow to discuss case for acceptance to Cardiology service
- ED will page MICU resident once Cardiology fellow has accepted patient for admission
- Cardiology fellow will document Plan of Care in EPIC for any patients not accepted to Cardiology service
- MICU resident will evaluate patient, place admission orders and write documentation for each admission
- MICU resident will staff all CCU admissions with on-call Cardiology fellow. Telemetry admissions can be staffed in the following morning
- MICU resident will also staff all CCU admission with ICU nocturnist. Nocturnist may see patients together with resident, or independently, at their discretion
- See Admission Workflow under Cardiac Care Unit (CCU) above for additional details
- Rapid Response/Code Blue
- MICU night float senior resident will carry RRT/Code Blue pager at all times during overnight hours (6:00PM-6:00AM)
- MICU senior resident (along with ward night float crosscover resident) will respond to all RRT and Code Blue called in hospital
- Following RRT or Code Blue, either MICU or wards night float resident will document events in EPIC
B. ICU Procedure Policy
- All procedures performed overnight follow same policy as in MICU
- See ICU Procedure Policy under Medical Intensive Care Unit (MICU) above
II. Rotation LogisticsMedical Intensive Care Unit (MICU)A. Team Composition
- MICU team will be composed of:
- Attending intensivist
- Pulmonary/Critical Care fellow
- 2-3 senior residents, may include off-service residents (Emergency Medicine, Anesthesia, visiting residents)
- 3-4 interns, may include off-service residents (Emergency Medicine)
- 1-3 subinterns (4th year medical students)
B. Daily Schedules
| 6:00AM |
AM Signout (MICU Workroom) |
| 7:00-9:00AM |
Prerounds |
| 9:00-12:00PM |
Attending Rounds |
| 12:00-1:00PM |
Noon Conference* |
| 1:00-5:00PM |
New admits, patient care |
| 6:00PM |
PM Signout |
*Optional for residents on MICU rotation
C. Day Off Policy
- Days off for all MICU interns and residents are pre-assigned to ensure appropriate coverage at all times
- Unless unavoidable, interns and residents will NOT be scheduled for same day off to ensure appropriate continuity of care
- Residents, including off-service residents, may email UCI Administrative Chief with specific day off requests. Requests should be submitted at least 30 days prior to start of rotation, or by no-call request deadline
Cardiac Care Unit (CCU) A. Team Composition
- CCU team will be composed of:
- Attending cardiologist
- Cardiology fellow
- 1 senior Medicine resident
- 2 interns
- 1-2 subinterns (4th year medical students)
B. Daily Schedules
- CCU rotation follows same daily schedule as MICU
- See Daily Schedule under Medical Intensive Care Unit (MICU) above
C. Day Off Policy
- Days off in CCU are not pre-assigned, and may be taken off as desired, following discussion with remainder of team members
- Senior residents are encouraged to not take weekend days off, if possible, given covering fellow also covering consult service, inpatient stress tests, etc.
MICU/CCU Night Float A. Team Composition
- Night float team comprised of:
- ICU nocturnist
- 1 senior Medicine resident
- 1 intern
B. Daily Schedules
| 6:00PM |
PM Signout (MICU Workroom) |
| 6:00-6:00AM |
Admissions, patient care |
| 6:00AM |
AM Signout |
C. Rotation Schedules
- Seniors
- Senior residents will work five days per week, with one post call day and one day off (see below)
- Jeopardy senior resident will cover MICU night float two nights per week
- Each jeopardy resident may cover one or both ICU nights depending on the number of seniors on jeopardy, at discretion of senior backup chief resident
- Interns
- Interns will work five days per week, with one post call day, and one day off (see below)
- Jeopardy or elective interns will cover MICU night float two nights per week
D. Day Off Policy
- Days off are pre-assigned to both seniors and interns on night float rotation
- Seniors: Post-call Wednesday, day off Thursday night each week
- Interns: Post-call Saturday, day off Sunday each week
E. Call Rooms
- Call rooms are located in the 7200 unit (rooms 7241 and 7243)
- Rooms are equipped with mattress, computer and phone
|